Purpose: Skeletal muscle ischemia reperfusion injury (IRI) remains a clinical challenge in orthopaedic and trauma practices. There is limited consensus on the optimal model or methodology to study IRI effects on extremity function in vivo. Most studies have used the mouse hindlimb, which does not reflect the anatomical or functional complexity of the upper extremity. The purpose of this study was twofold: (1) to establish and validate a reproducible model of tourniquet-induced extremity IRI, and (2) to investigate the impact of upper limb tourniquet use in upper extremity function.
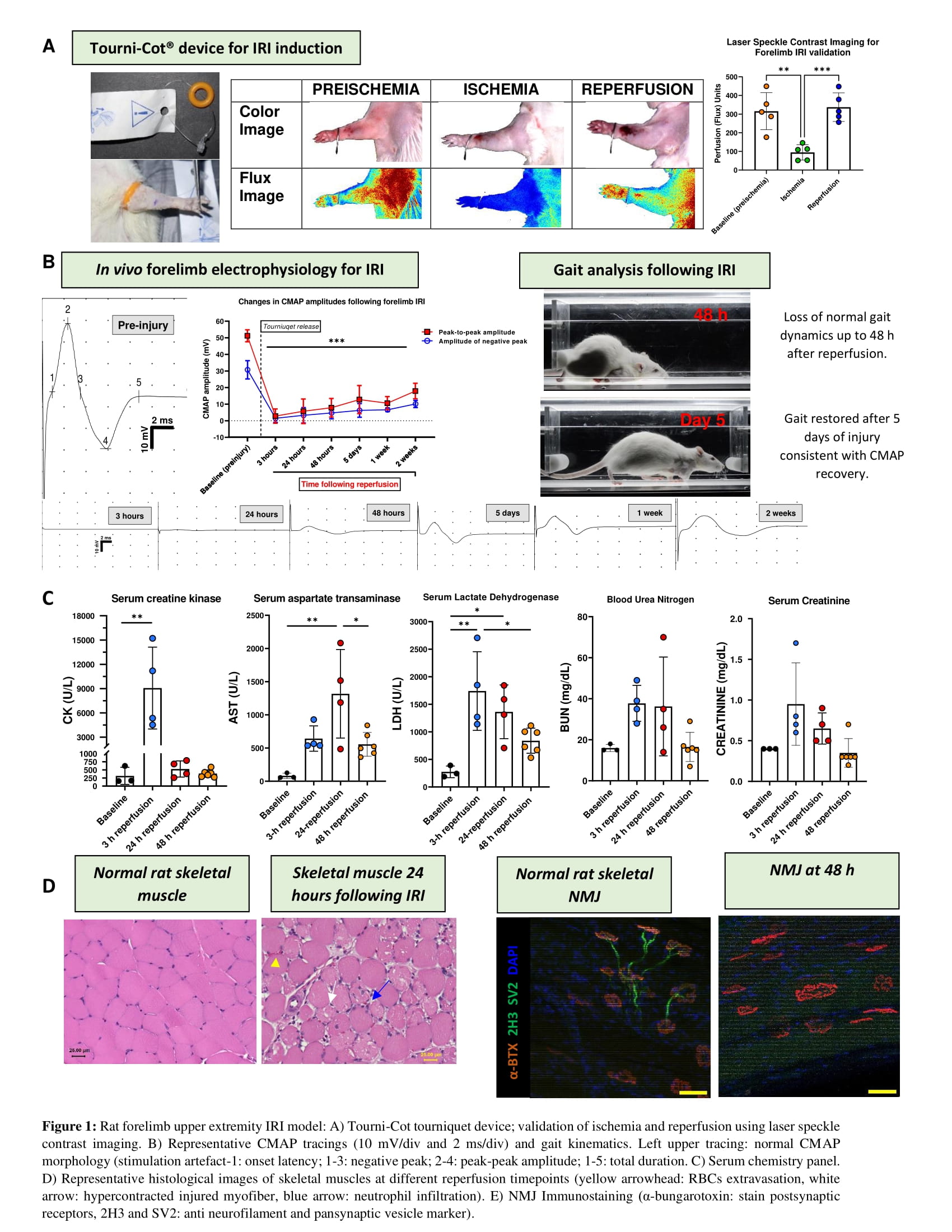
Methods: A unilateral tourniquet-induced IRI (2.5 h ischemia time) was established in the forelimb of Sprague-Dawley rats using a commercially available exsanguinating device. Ischemia and reperfusion were confirmed both clinically and quantified using laser speckle contrast imaging. Functional evaluation was performed using gait kinematics and in vivo electrodiagnostic studies at different reperfusion timepoints. Compound muscle action potential (CMAP) was evoked by incremental and supramaximal stimulation of the brachial plexus using current intensity of 1-20 mA; frequency, 10Hz; filter settings, 1 Hz-10kHz. Serum biochemical markers of muscle injury were evaluated using automated chemistry analyzer. Histological staining and neuromuscular junction immunostaining were also performed.
Results: Tourniquet application resulted in significant reduction in forelimb perfusion (P = 0.0013) and its release re-established baseline flow (P = 0.0006). Significant differences were found between CMAP negative peak amplitude and area compared to baseline parameters up to 2 weeks post-IRI (P <0.0001). No significant difference was seen between onset latency across all time points following reperfusion (P>0.1). Serum Creatine Kinase was significantly higher following 3-hour reperfusion (P = 0.011). Serum lactate dehydrogenase was statistically significant both following 3-h (P = 0.002) and 24-h reperfusion (P = 0.0161). Neuromuscular junction immunohistochemistry revealed denervation at both 24 and 48 h following reperfusion. Histological analysis revealed polymorphonuclear infiltrates and sarcoplasm loss.
Conclusion: A forelimb rat IRI model presented here could provide functional insights and elucidate electrophysiologic alterations associated with upper extremity tourniquet use. Nerve conduction study and immunohistochemistry findings are consistent with conduction block and denervation, respectively. The CMAP size, represented by amplitudes and areas of the biphasic waveform, represents a sensitive and clinically applicable parameter for evaluating post-tourniquet induced-IRI denervation recovery. Gait analysis could be useful in later time points following IRI induction.


{kind=link}