Purpose: The aim of the study was to investigate the relationship between the standard sagittal starting point for insertion of TINs (tibial intramedullary nails) and the tibial axis on the sagittal plane.
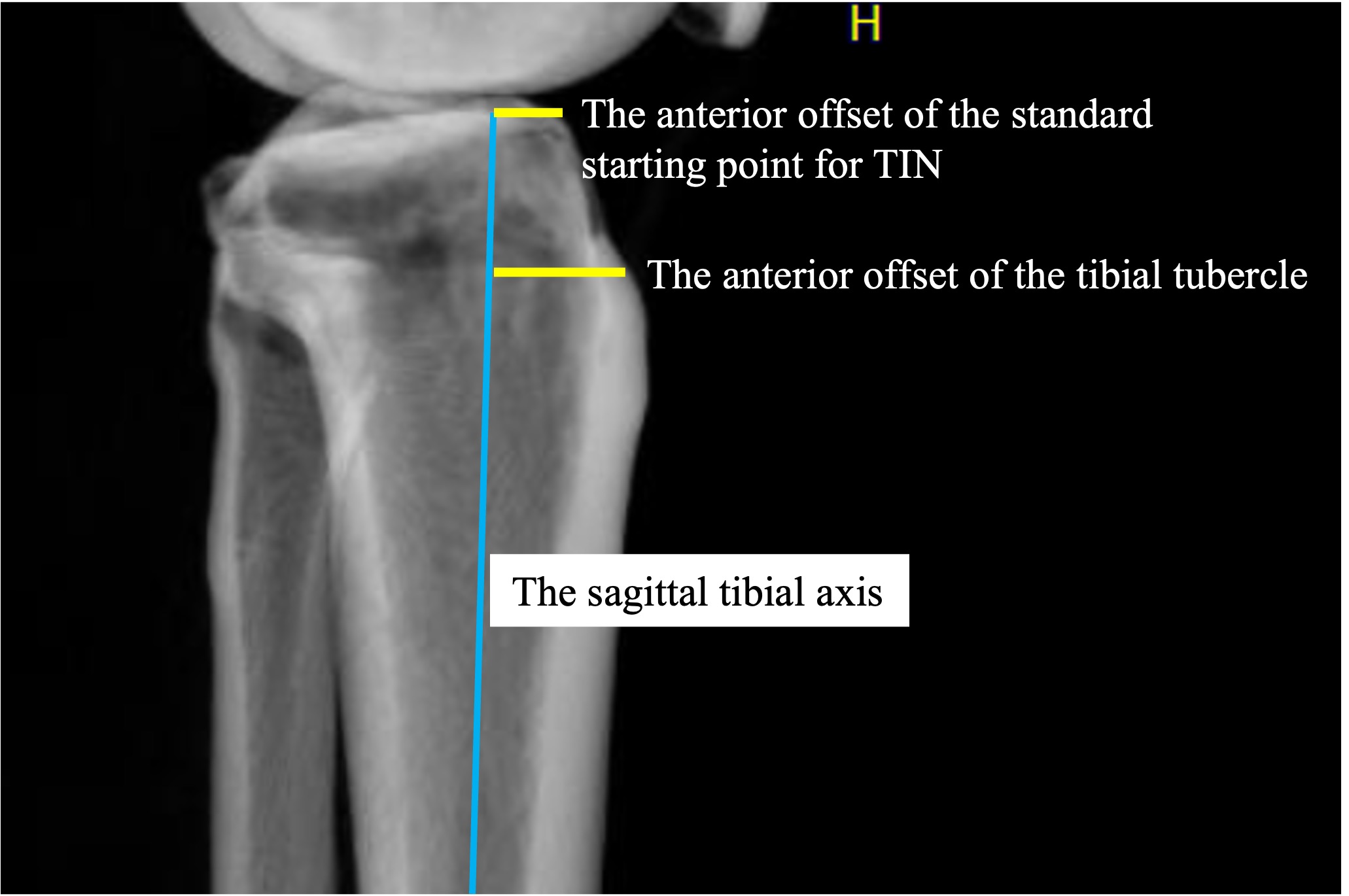
Methods: Adult inpatients who underwent tibial CT scans between 2019 and 2022 were included in the study. The male-to-female ratio and the distribution of patients’ ages were manually equalized. A total of 50 male and 50 female patients (mean age: 52.7 years) were included, with all but one being of Asian descent. Transparent 3D images that replicated the lateral radiographic view of the tibia were created to measure the anterior offset from the sagittal tibial axis to the standard sagittal starting point for TINs, as well as the tibial tubercle. Additionally, the tibial length, the diameter of the isthmus, and the distance from the center of the isthmus to the tibial end (expressed as the ratio in relation to the tibial length) were evaluated.
Results: The median anterior offset from the tibial axis to the starting point was 9.8 mm (interquartile range [IQR]: 7.2 to 12.2 mm). The median anterior offset of the tibial tubercle was 16.7 mm (IQR 14.6 to 18.9 mm). The median distance from the anterior edge to the tubercle was 24.5 mm (IQR: 22.5 to 26.6 mm). The median length of the tibia was 330.4 mm (IQR: 314.3 to 341.2 mm). The median diameter of the isthmus was 10.4 mm (IQR: 8.9 to 11.8 mm). The median ratio of the isthmus in the tibial length was 39.7% (IQR: 38.2% to 41.3%). There was a weak correlation between the anterior offset of the starting point and age (r = 0.24, P = 0.016). Seven cases (7%) had the anterior offset of less than 5 mm from the tibial axis to the starting point due to anterior bowing of the tibiae. No significant differences were observed between males and females regarding the anterior offsets and diameter of the isthmus.
Conclusion: The median anterior offset from the tibial axis to the starting point was less than 10 mm, with 7% of cases having an offset of less than 5 mm. Surgeons should be cautious when dealing with cases with a small anterior offset, as it may pose challenges during TIN insertion or result in postoperative malreduction at fracture sites.

 photo")
{kind=link}